Introduction
In the last two decades, executive function (EF) has piqued the interest of several researchers in the field of education, psychology, and language learning and development. This relatively new area of research has significant impact on social development and academic achievement in children, as well as on how individuals apply and use knowledge in everyday life in adulthood (Henry, 2015). Executive function is not a unitary concept; it is an umbrella term that denotes various cognitive functions including working memory, inhibitory control and cognitive flexibility (Elliot, 2003). Language learning is closely linked to higher cognitive functions, the evidence for which can be drawn from research findings (Singer and Bashir, 1999; Bernier et al, 2012; Corbett et al, 2009; Lambeth and Liesen, 2011; Trainor, 2010). Moreover, some researchers (Henry et al, 2012; Figueras et al, 2008; Carney et al, 2013) have found significant EF deficits across a range of clinical groups when compared with typically developing children. It is of paramount importance that Speech and Language Therapists working in school settings have a reasonably good understanding of the reciprocal relationship between executive functions and language (Singer & Bashir, 1999), EF disorders and how these could further inform interventions in clinical practice. Hence, examining the research evidence for EF disorders and implementing evidence-based interventions to facilitate the development of executive functions is imperative.
An attempt has been made here to explore the relation between language and executive functions from studies on typical development, and EF deficits in children with special needs. Moreover, some clinical implications and potential steps for future research projects have also been discussed.
Executive Functions: definitions, related terms and measures
Executive functions are the cognitive processes involving decision-making and planning that are elicited when faced with new challenges (Singer & Bashir, 1999).
Diamond (2013, p. 1) describes ‘core EFs as inhibition [response inhibition (self-control – resisting temptations and resisting acting impulsively) and interference control (selective attentions and cognitive inhibition)], working memory, and cognitive flexibility (including creatively thinking “outside the box”, seeing anything from different perspectives, and quickly and flexibly adapting to changed circumstances).’ This has been illustrated in Fig 1.
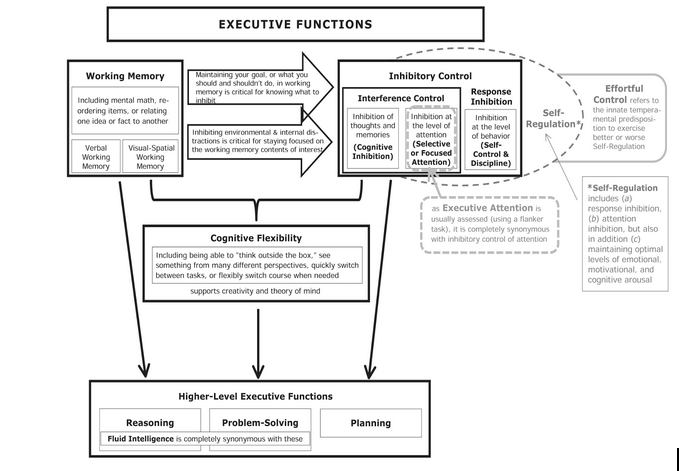
Fig 1: Executive functions and related terms (Source: Diamond, 2013)
Inhibitory control involves acting appropriately (or as needed) by controlling one’s attention, thoughts, emotions and behaviours in the presence of a strong internal predisposition or external lure (Diamond, 2013). From their longitudinal study, Moffitt et al (2011) demonstrated that inhibitory control in early life could predict outcomes in adulthood i.e. children (from ages 3 to 11 years) who had better inhibitory control were more likely to be in school as teenagers, less likely to smoke or take drugs, and had better physical and mental health as adults. Working Memory (verbal and visual-spatial) requires holding information in the mind and working with it mentally (Smith and Jonides, 1999). Working memory (WM) forms the foundation skills for reasoning, critical thinking and creativity (Diamond, 2013). Cognitive flexibility, which builds on inhibitory control and working memory, develops much later in life, and requires the ability to adapt to changes and demands. Children succeed in cognitive flexibility tasks usually around 41/2 -5 years (Diamond, 2013).
The neuronal basis of executive function has been assessed by neuroimaging techniques. Duncan and Owen (2000) observed a clustering of frontal lobe activations for a wide range of executive function tasks in various studies. Their findings suggest that there could be some functional segregation in the prefrontal regions. Despite the fact that executive function and frontal lobe function are often used interchangeably, recent theories suggest that posterior cortical regions and subcortical structures may also be involved to mediate the processing of executive functions (Rebecca, 2003).
Although several tests are available to measure EFs (which are closely related to one another), one might question which component of EF a task might require (Diamond, 2013). Some of the psychological measures used to assess EF have been summarised in Fig 2.
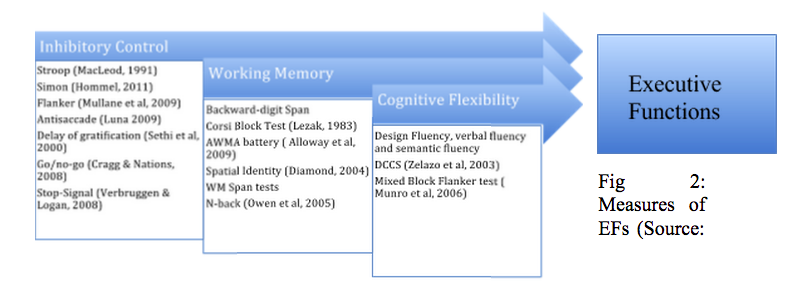
Fig 2: Measures of EFs (Source: Diamond, 2013)
Executive Functions and Language
In their pioneering work, Bernier et al (2012) investigated links between quality of environment (in early years between 1 and 2 years) and executive function performance at the age of 3 years in typically developing children. Parent-child interactions form the core of a young child’s development during the first few years of life (including the development of executive functioning); however, research evidence for the role of social factors is scarce. Sixty-two families (38 girls and 24 boys) were randomly selected from a large Canadian metropolitan area for this study. Caregiving relationships were assessed on the quality of parent-child interactions (maternal sensitivity, mindfulness, autonomy-support, and quality of father-child interactions) and security of the mother-child attachment relationship. Results suggested that attachment security was more relevant in predicting EF and higher-quality parenting was associated with better EF performance. Cognitive flexibility was also linked to children’s verbal ability amongst other factors. Moreover, these researchers suggested that gene-environment interactions must be taken into consideration and recommended family involvement in intervention programmes aimed to improve executive functions in young children.
Metacognitive strategies (self-regulation, monitoring, planning and executing tasks appropriately) are essentially mediated with language. In the early years of development, children talk to themselves about the activities they are engaged in (private speech), which is eventually internalised (inner/internal speech) when they grow older (Vygotsky, 1964). The social context and academic experiences help shape these metacognitive strategies, which are largely based on the development and use of language (Singer & Bashir, 1999). In their case study of a 16-year old boy with difficulties in speech production, word retrieval, language formulation, executive functions (planning, sustaining focus etc.), and self-regulation (regulate communication effectively), Singer & Bashir (1999) demonstrated that interventions addressing the reciprocal influences of executive functions, self-regulation and language had promising results.
Trainor (2010) studied the relationship between executive functions and narrative ability in pre-schoolers (19 children, aged 4-5 years) using Peabody Picture Vocabulary Test for receptive language, Renfrew Bus Story for oral narrative language and Behaviour Rating Inventory of Executive Function (BRIEF) for inhibition, WM, flexibility and planning. The author found strong correlations between oral narratives and EFs, especially for metacognition that involves working memory and planning, demonstrating a link between expressive language and executive functions. Similarly, Lambeth and Liesen (2011) demonstrated a strong relationship between BRIEF and narrative language ability when they examined the relationship between language and executive functions in school-aged children. The authors have suggested that storytelling and discourse involve inhibitory control, organisation, flexibility and planning, hence corroborating previous research findings.
Although researchers have contemplated on which aspects of cognitive development are more independent of language development and vice versa (Morgan, 2015), it is apparent that the link between EF and language is undeniable. In the early years of speech and language development, the caregiving environment is an essential pre-requisite in the development of language and EF skills. Joint attention skills (sharing attention with others by showing, pointing and coordinated looking between object and people) are crucial for language development (Kasari, 2006). In the preschool years, children use metacognitive strategies (which involve working memory, planning), cognitive flexibility and inhibitory control for story telling and expressive language (Trainor, 2010). They often rely on ‘self-talk’ strategies for tasks involving problem solving. From this point onwards, there seems to be a reciprocal relationship between EF and language, especially as regards tasks involving verbal reasoning, making inferences and discourse. Moreover, the ability to reflect on language (metalinguistic awareness), which requires appropriate EF skills (Morgan, 2015), facilitates language development in children.
The link between language and executive functions has been investigated in children with EF disorders (atypical development), some of which are reviewed in the following section.
Current Research in EF disorders in children
Research in EF disorders was initiated primarily in the area of Specific Language Impairment (SLI). Several researchers have studied executive functions in children with ASD, ADHD, William’s syndrome, Down syndrome, as well as deaf children. Some of these studies are illustrated in Figure 3.
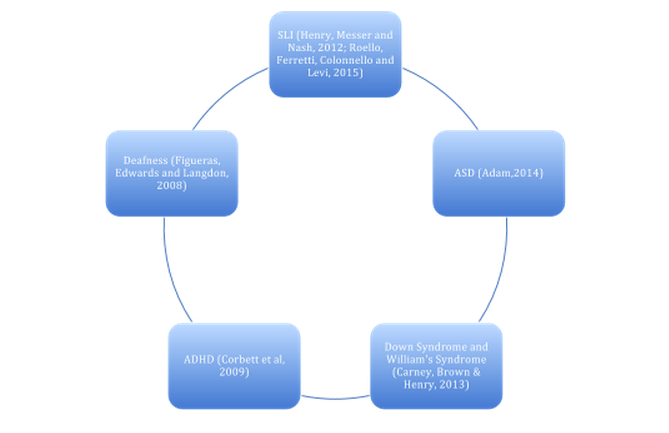
Fig 3: Some studies in EF disorders in children
Henry et al (2012) investigated whether children with SLI (n= 41) had poorer EF skills compared to typically developing children (n= 88). Participants who did not meet the inclusion criteria for SLI or the typical control group were put in the Low Language Fluency group (n= 31). Using a battery of tests, the researchers examined if EF difficulties were confined to language-based tasks or whether they extended to non-verbal tasks. Children with SLI showed difficulties with executive-loaded working memory, fluency, planning and inhibition on both verbal and non-verbal tasks. From their findings, they concluded that individuals with SLI had severe but widespread executive function difficulties, which were not confined to the language domain. Children in the Low Language Fluency group had significant EF difficulties suggesting a link between moderate language impairment and EF skills.
Roella et al (2015) investigated EF performances in two age groups (young: mean = 53.6; old: mean= 65.4) of pre-schoolers with SLI (N= 60) and without SLI (N= 58) using various measures. Children with SLI scored lower on categorisation and shifting tasks than typically developing children. Moreover, they had specific difficulties in problem representation and cognitive flexibility. Although EFs improved with age, the performance of children with SLI remained lower than the typically developing group. The authors concluded that children with SLI had more difficulties with planning at 65.4 months due to limited language abilities. Pre-school children with SLI had EF impairments in problem solving and inhibitory control, which may be due to difficulties in using inner speech for mental representations required in these tasks. This study lends support to previous theories on child development, and suggests that preschool aged children with SLI have significant difficulties using language for reasoning.
Adam et al (2014) examined the relation between EFs and language ability in children with autism (62 children, aged 8-10 years, 47 males and 15 females) using correlational and regression analyses in measures for cognitive ability, ASD symptomatology, language abilities and executive functions. Their results indicated that core language ability and pragmatic language ability significantly predicted the children’s performance on direct measures of working memory. This could differentiate these children from children with SLI who might have EF deficits in inhibition, mental flexibility and organisation.
Carney et al (2013) compared EF skills across a range of verbal and visuospatial measures in children with Down syndrome (DS) and William syndrome (WS) to those of typically developing matched children. Children with DS had particular difficulty in WM tasks on both verbal and non-verbal measures whereas switching was impaired in the verbal domain. Children with WS had far more difficulties with EF indicating a general EF weakness with specific difficulties in non-verbal EF tasks. Inhibition measures in both domains were affected which could cause problems in behavioural control leading to academic and social difficulties.
Corbett et al (2009) carried out an extensive study to compare six domains of EF in children with ASD, ADHD and typically developing children. Children with autism had lower scores in inhibition, working memory, flexibility and vigilance as compared to the typically developing children. Although there were no statistically significant differences across the two clinical groups in planning and fluency, children with ASD performed more poorly in inhibition, working memory and flexibility as compared to children with ADHD. The authors highlighted the overlap as well as the distinctions between ASD and ADHD resulting in significant implications in diagnosis and treatment of these conditions.
Figueras et al (2008) compared EF and language skills of implanted (N=22) and non-implanted pre-lingual deaf children (N=25) born to hearing parents with those of age-matched hearing children (N=22). Measures included a battery of tests for EF (planning, shifting, working memory, impulse regulation and visual attention), British Picture Vocabulary Scale for receptive vocabulary and Test for Reception of Grammar-version 2 for assessing receptive grammar. Additionally, they examined the association between language and EF in these groups. The results suggest a high correlation between language ability and EF in both hearing and deaf children, but there were no differences between the implanted and non-implanted deaf groups.
Although one would expect language skills to be better in children with cochlear implants as opposed to children with hearing aids, this advantage was not supported by their research findings. The authors attributed this to the fact that the children with cochlear implants had more severe hearing losses and had lesser time (limited device use) to catch up on their language development as compared to children with hearing aids. Moreover, they suggested that deaf children find it difficult to use internal speech in order to hold the task rules in working memory and to plan and regulate behaviours. Significant differences emerged in the card sorting game indicating that language difficulties in deaf children resulted in difficulties in cognitive flexibility. Planning and problem solving skills were not compromised on visual-perceptual tasks, which were independent of language skills. Hence it was concluded that EF deficits in deaf children were linked to delayed language acquisition and cannot be attributed to deafness.
On examining studies on EF disorders through a critical lens, a strong correlation between language difficulties and executive function deficits has emerged. Children with special needs from various clinical groups had statistically significant deficits in executive functions as compared to typically developing children. Children with SLI had wider executive function difficulties that were not limited to verbal tasks revealing a widespread EF deficit. Children with deafness had EF difficulties in the verbal domain, not in tasks that are independent of verbal ability, indicating that their underlying difficulty in internal speech resulted in these EF deficits. Pragmatic language ability in children on the autism spectrum could predict working memory performances. Children with ADHD showed significant EF difficulties in a range of measures as compared to typically developing children. Similarly, children with DS had more difficulties with WM tasks and in switching on verbal tasks whereas children with WS had more general difficulties on inhibition measures with specific difficulties in non-verbal tasks. Although small sample size may pose as a limitation in some of the aforementioned studies, these research findings offer overwhelming evidence for links between language and EF in these clinical groups.
Clinical Implications
From a Speech and Language Therapist (SLT)’s perspective, it is evident that the individual needs of children with EF disorders can only be addressed by developing child-centred intervention programmes using a multidisciplinary approach involving educational psychologists, special educators as well as caregivers. SLTs should probably use tests for measuring wider executive functions in addition to language assessments (Lambeth and Liesen, 2011).
In her extensive review of research on cognition in monolingual and bilingual children, Bialystok (2001) concluded that bilingual children had a cognitive advantage, which was further demonstrated in recent research comparing executive functions in bilingual and monolingual children (Bialystok and Vishwanathan, 2009). Carlson and Meltzoff (2008) found similar advantages in bilingual children in their ability to manage conflicting attentional demands as compared to their monolingual counterparts. They attributed this advantage to ‘thinking in two languages’ where bilingual children had to hold in mind the relevant language whilst inhibiting the non-relevant one.
Since results of static language assessments standardised on monolingual English speaking children cannot be applied to culturally and linguistically diverse populations, examining executive functions in bilingual children could offer some insight into their language skills. Henry et al (2012) found that children with SLI have a general executive function deficit in both verbal as well as non-verbal tasks. Hence, tests measuring EF difficulties in bilingual children could potentially determine developmental language impairment (which may be overlooked if testing procedures did not include assessment of EFs) and aid in differential diagnosis as well as planning appropriate interventions in this population. A battery of tests including speech and language assessments, dynamic assessments and executive functions could help differentiate language impairment from differences due to linguistic context. Consequently, strategies that help improve metacognitive skills would have a strong impact on language learning and development.
Children with ASD, ADHD, deafness, William syndrome and Down syndrome have significant EF deficits as compared to typically developing children. Differential intervention approaches over and above language interventions would be required to cater to their individual needs (Adam, 2014). Improving working memory is crucial for children with Down syndrome as they learn new information and apply this to structured tasks (Carney et al, 2013). As regards deafness, intervention should consider EF deficits and how these could affect the children in the long run, both socially as well as academically. Teaching deaf children to implement ‘self-talk’ strategies for planning and problem solving may foster improvement in EF skills (Figueras et al, 2008).
Implementing interventions (CogMed, task switching etc.) that have a reasonable evidence base is the need of the hour (Diamond, 2013). Working memory intervention could be considered as a viable option in developmental disorders (Henry, 2015). However, lack of clinical knowledge/skills and insufficient evidence for treatment efficacy (a meta-analysis by Melby-Lervåg & Hulme, 2013 suggests no transfer of function for working memory interventions) may pose as barriers to evidence-based practice. Hence, overcoming these barriers by critically reviewing research findings as well as participating actively in clinical research is absolutely necessary. This would in turn ensure high standards of service provision, duty of care being central to clinical practice.
Conclusion
Based on current research findings, the link between language and EF is clearly evident. Since children in each clinical group present different profiles of EF deficits, child-centred interventions that cater to their individual needs should be incorporated in speech and language therapy. Future research projects could explore the potential of using EF measures in a battery of speech and language tests for differentiating language impairment from differences due to linguistic context in children from culturally and linguistically diverse populations.
Considering the fact that the pre-frontal cortex (which is essentially responsible for EFs) takes much longer to develop, executive function can be improved at any age using a range of programmes and interventions (Mason, 2015). Although there is a high correlation between EF intervention and academic achievements, causal links have not been fully established (Jacob & Parkinson, 2015). Hence, it becomes necessary to examine the efficacy of EF intervention programmes using rigorous research methods (randomised control trials), and implement evidence-based practice while addressing the needs of children with developmental disorders. Additionally, further research to explore long-term effects of EF interventions on the development of language in children with special needs is warranted.
References
Adam W. McCrimmon (Commentary author) (2014). A relation between executive functions and language ability in children with ASD that has implications for intervention. Evidence-Based Communication Assessment and Intervention, 8:1, 5-8.
Bialystok, E. (2001). Bilingualism in development: Language, literacy, and cognition. New York: Cambridge University Press.
Bialystok, E., & Viswanathan, M. (2009). Components of executive control with advantages for bilingual children in two cultures. Cognition, 112(3), 494-500.
Bernier, A., Carlson, S. M., Deschênes, M., & Matte‐Gagné, C. (2012). Social factors in the development of early executive functioning: a closer look at the caregiving environment. Developmental science, 15(1), 12-24.
Carlson, S. M., & Meltzoff, A. N. (2008). Bilingual experience and executive functioning in young children. Developmental science, 11(2), 282-298.
Carney, D. P., Brown, J. H., & Henry, L. A. (2013). Executive function in Williams and Down syndromes. Research in developmental disabilities, 34(1), 46-55.
Corbett, B. A., Constantine, L. J., Hendren, R., Rocke, D., & Ozonoff, S. (2009). Examining executive functioning in children with autism spectrum disorder, attention deficit hyperactivity disorder and typical development. Psychiatry research, 166(2), 210-222.
Diamond, A. (2013). Executive functions. Annual review of psychology, 64, 135-168.
Duncan, J., & Owen, A. M. (2000). Common regions of the human frontal lobe recruited by diverse cognitive demands. Trends in neurosciences, 23(10), 475-483.
Figueras, B., Edwards, L., & Langdon, D. (2008). Executive function and language in deaf children. Journal of Deaf Studies and Deaf Education;13:362-377.
Henry, L. A., Messer, D. J., & Nash, G. (2012). Executive functioning in children with specific language impairment. Journal of child psychology and psychiatry,53(1), 37-45.
Henry, L. A. (2015). Executive Functions and Every Day Life – Children with Developmental Disorders. Dean’s Lecture Series, School of Health Sciences, City University.
Jacob, R., & Parkinson, J. (2015). The Potential for School-Based Interventions That Target Executive Function to Improve Academic Achievement A Review. Review of Educational Research. Downloaded from RER.net Extracted on 30.04.15
Kasari, C., Freeman, S., & Paparella, T. (2006). Joint attention and symbolic play in young children with autism: A randomized controlled intervention study. Journal of Child Psychology and Psychiatry, 47(6), 611-620.
Lambeth, S., & Liesen, J. (2011). ‘Relationship between School-Age Executive Function and Language Skills.’ ASHA Convention 2011. Available at Asha.org (Extracted in March 2015)
Liesen, J. (2011). ‘The Relationship Between Executive Function and Language Abilities in Grade School Children.’ [PowerPoint Presentation] Available at Slide Serve (Extracted in March 2015)
Mason, K. (2015). ‘Executive Functions and Deafness.’ [PowerPoint Presentation] HCM019: Language Learning and Development. Available at Moodle City (Extracted on 4.3.2015)
Melby-Lervåg, M., & Hulme, C. (2013). Is working memory training effective? A meta-analytic review. Developmental Psychology, 49(2), 270.
Moffitt, T. E., Arseneault, L., Belsky, D., Dickson, N., Hancox, R. J., Harrington, H., … & Caspi, A. (2011). A gradient of childhood self-control predicts health, wealth, and public safety. Proceedings of the National Academy of Sciences, USA.2011; 108:2693-98.
Morgan, G. (2015) ‘Language Cognition Dependencies.’ [PowerPoint Presentation] HCM019: Language Learning and Development. Available at Moodle City (Extracted on 4.3.2015)
Roello, M., Ferretti, M. L., Colonnello, V., & Levi, G. (2015). When words lead to solutions: Executive function deficits in preschool children with specific language impairment. Research in developmental disabilities, 37, 216-222.
Sarver, D. E., Rapport, M. D., Kofler, M. J., Scanlan, S. W., Raiker, J. S., Altro, T. A., & Bolden, J. (2012). Attention problems, phonological short-term memory, and visuospatial short-term memory: Differential effects on near-and long-term scholastic achievement. Learning and Individual Differences, 22(1), 8-19.
Smith, E. E., & Jonides, J. (1999). Storage and executive processes in the frontal lobes. Science, 283(5408), 1657-1661.
Singer, B. D., & Bashir, A. S. (1999). What are executive functions and self-regulation and what do they have to do with language-learning disorders? Language, Speech, and Hearing Services in Schools, 30(3), 265-273.
Trainor, K. (2010). ‘The relationship between preschool executive function skills and oral narrative skills.’ [PowerPoint Presentation] Unpublished manuscript, Department of Communication Disorders and Sciences, Eastern Illinois University, Charleston, Illinois. Available at Slide Finder (Extracted on 8.4.15)
Vygotsky, L. S. (1964). Thought and language. Cambridge, MA: MIT Press.
Written by Sai Bangera, Speech and Language Therapist